WARNING: THIS NOTE IS HUGE AND MESSY!
Functions of Cardiovascular system:
- maintains adequate blood flow to all body tissues
- rapid-transport system for gases, specialized cells, nutrients and waste
- keeps blood pressure within normal limits
- provides rapid adjustment to changes in demand
- temperature and fluid regulation




 | |
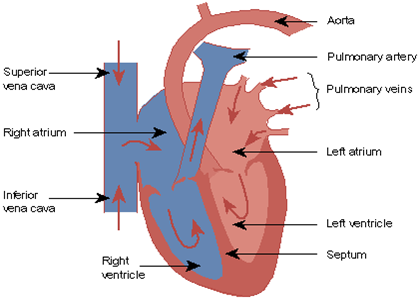
| Structure of the heart |
 | |
| Neural Connections |
- Right atrium and ventricle = right pump => pulmonary circuit
- Left atrium and ventricle = left pum => systemic ciruit
- Atria and ventricles separated by connective tissue ring
- Heart wall consists of four layers (Peri-, Epi-, Myo-, Endo - cardium)
- Myocardium consists of striated branched cells with intercalated discs = ''functional syncytium''
- Energy efficient tissue
Microanatomy:
- Short fat branching cells
- One large central nucleus per cell
- Intercalated discs
- Gap junctions
- Myofibril-like units
- High capillary density
- Large number and size of mitochondria
- Large sarcoplasmic reticulum and T.Tubule system

- Conduction system = specialized cells that initiate and distribute electrical impulses to ''contractile'' cells
- Sinoatrial (SA) node contains pacemaker cells that establish the heart rate (across atria). Connects to atrioventricular (AV) node via 'internodal' pathways. The impulse travels down the bundle of His and splits into right and left bundle branches. The impulse is then distributed rapidly by Purkinjie fibres to ventricular muscle.

 Mechanical events:
Mechanical events:- Cyclical contraction (systole) and relaxation (diastole) relating to emptying and filling periods.
- Total time = 0.8s of which Systole = 0.3s, Diastole = 0.5s
Heart Simulation link: the pressure and volume changes over the duration of a complete cardiac cycle. Normal blood volume is 5-6 litres. The rate blood volume circulates the body is measured by the cardiac output.
Cardiac output: is the volume of blood (ml or L) pumped out of the left ventricle per minute.
Stroke volume(ml/beat) x Heart rate (beats/min) = Cardiac output (l/min)
During Rest/Exercise 80/100 75/150 6/15
Cardiac output distribution at rest and exercise:
Brain = 14% 14% Heart = 4% 5% Skeletal muscle = 21% 60% Skin = 5% 15% Kidneys = 20% 2% Liver and GIT = 27% 2% Other = 9% 2%
Factors affecting heart rate:
- Normal pacemaker activity = 80-100 b/min
- Parasympathetic decreases HR = 70-80 b/min: via acetyl choline (ACh) acting on SA node cells
- Sympathetic increases HR via Norepinephrine (NE) acting on SA node cells
- Hormones epinephrine, thyroxine increase HR
Factors affecting Stroke volume
- The Frank-Starling principle: an increase in end-diastolic volume results in a greater stroke volume = increased ventricular filling causes increased ventricular stretch and causes increased contractile force. In other words, ''more in = more out''
- Sympathetic stimulation of receptors in cardiac muscle by norepinephrine (NE) from nerve fibres and epinephrine (E) from adrenal gland.
- Parasympathetic stimulation of SA and AV nodes by acetyl choline.
- Glucagon and thyroid hormones


NOW THAT WE KNOW SOME BITS ABOUT CARDIOVASCULAR PHYSIOLOGY LETS TALK ABIT ABOUT BLOOD PRESSURE
Organisation of the circulatory system
Vessel
Arteries ~4mm; (function=)distribute blood under high pressure to internal organs.
Arterioles ~30um; change in response to local, nervous or endocrine stimulation
Capillaries ~8um; permit efficient exchange between blood and other mediums
Venules ~20um; collect blood from capillary beds
Veins ~5mm; transport blood with the aid of valves

- Blood Pressure (BP) is the pressure exerted by the blood against a vessel wall and it depends on the volume of blood and the resistance within the vessel. The volume of blood entering and leaving the arteries is not constant during heart contraction (systole) and relaxation (diastole). BP is separated into systolic (high) and diastolic (low). Systemic BP is greater than pulmonary BP.
Normal values
Systemic Arterial:
 Systolic BP=120mmHg
Systolic BP=120mmHgDiastolic BP=80mmHg
Pulmonary Arterial
Systolic BP=25mmHg
Diastolic BP=8mmHg

Mean Arterial Pressure (MAP) = Diastolic + (0.33*(Systolic-Diastolic))
e.g. 80 + (0.33* (120-80)) = 93mmHg (93mmHg is a normal MAP)
Control of BP and flow
- Blood flow through tissues depends on the pressure gradient and vascular resistance. Blood flows from high to low pressure down a pressure gradient (higher gradient=increased flow). Changes in diameter of arterioles affects blood flow and blood pressure. Blood pressure inceases when the diameter of arterioles decreases and vice versa

Control of blood pressure
Decrease in blood pressure => causes decrease stimulation of baroreceptors => medulla cardiovascular centre => decrease parasympathetic stimulation of the heart => increase sympathetic stimulation of heart, arterioles, veins => increase in blood pressure
Factors affecting blood pressure: blood volume, heart rate, stroke volume, blood viscosity, peripheral resistance
Mean arterial pressure is determined by
Cardiac Output x Total Peripheral Resistance
i.e. Blood pressure increases when:
- blood volume increases and/or
- Heart rate increases and/or
- Stroke volume increases and/or
- Blood viscosity increases and/or
- Peripheral Resistance increases and/or

{kind=link}

THE FOLLOWING WERE TAKEN FROM SECOND YEAR
Lecture 1. The structure of the
Cardiovascular System:
Review of functions and structure of
cardiovascular system. Structure of heart. The layers of the heart, special
properties of the myocardium, pressure differences in different chambers of the
heart. Blood, brief overview of its constituents. Structural and functional
differences between different blood vessels. Microcirculation. Differences
between capillaries and lymphatic vessels, oedema.
Heart-
General structure: It is located in the middle mediastinum of thorax; the
apex of the heart is at the level of the fifth intercostal space; size of
average fist.
4
chambers, 2 thin atria, 2 thick ventricles (LV= 8-10 mm, RV= 2-3 mm); the atria are
separated by the interatrial septum whilst the ventricles are separated by the
interventricular septum. It contains valves between regions, e.g. AV valves (2
flaps-tricuspid on the right side and bicuspid on the left side) and also
semilunar valves (3 flaps). The flaps are held by connective tissue called the
chordae tendinae which are connected to the papillary muscles. Valves
are passive and only move due to pressure changes.
Three layers are found in the heart, a thin endocardium
(similar to endothelium of blood vessels), a thick myocardium and whole heart
is enclosed in pericardium (thin fibrous sheath, with interstitial fluid as
lubricant). The bulk of the heart is the myocardium, which consists of cylindrically shaped muscle
fibres with a rich supply of capillaries. The fibres are fused at regions
called intercalated disks which allow a low resistance pathway for ion
transport.
The contractile unit of the
heart muscle is the sarcomere, which consists of myofilaments called actin and
myosin which follow a sliding filament model of contraction. The tension developed
by the cardiac muscle depends on the cross bridges between actin and myosin and
thus the length of sarcomeres. As result of the tension generated during
systole, blood is ejected from the heart to the aorta.
On
each contraction of the heart, blood is expelled from the ventricles at high
pressure (Systolic = 120 mmHg, diastolic= 80 mmHg) into the aorta and pulmonary
artery. The expelled blood causes a rise in pressure in the aorta and distends
its wall. During diastole the tension in the aortic walls maintains flow of
blood onwards through the arteries, and the aorta diminishes in size until it
is again distended at the next heart beat.
Blood flows around the system due to i) pressure
difference ii) pumping of the heart iii) diastolic recoil of the arterial walls
iv) compression of veins by skeletal muscles and v) negative pressure in thorax
during inspiration.
Blood:e awvCVGBN
Our
body fluids can be split into extracellular (outside the cells) &
intracellular (inside the cells). The ECF can be split into the interstitial
fluid (fluid not in the vascular system but baths the cells, 10.5L) and the
blood (fluid in the vascular system, 3.5L). Blood is composed of red blood
cells (40-45%) suspended in plasma (55-60%), and is a medium for transfer of
heat, gases, proteins, glucose, waste products, fats, cellular debris. It is a
complex fluid, whose properties and composition changes. Blood volume
(RBC+plasma)= 5L, 70-75 ml/Kg body wt.; platelets= 2-3mm
diameter, 150000-300000/mm3; WBC= 5000-10000/mm3; RBC=
biconcave discs, diameter= 8mm,
thickness=2-4mm,
pigment Hb, 4.5-6 mill./mm3.
Also
contains proteins (Albumin, Fibrinogen); electrolytes (Na+, Cl-,
K+, Ca2+); Cholesterol, triglycerides, urea, creatinine,
glucose, uric acid. Produced in bone marrow by erythropoiesis.
Transport
System: The circulatory system is a closed system and can be
divided into 2 circuits, the pulmonary and systemic. The pulmonary circuit has less volume,
vessels are shorter and thin walled and lower pressure and less resistance. The
systemic circuit is a high pressure system and supplies and drains all the
organs and tissues of the body. Length of vessels decrease from Aorta to
venules, and then increase from terminal veins to vena cava. Thickness of
vessels decrease and then increase and the no. also increase and then decrease.
Velocity of blood is highest in aorta and decreases as the area of vessels in
the body increases.
Arteries:
There
are 2 types, elastic and muscular. The elastic predominate near the heart,
whilst the muscular are more towards the end of the arterial tree. They have 3
layers separated by elastic membranes,
a)
tunica intima- innermost layer, thin, surface of endothelial cells lying on a
basement membrane b) tunica media- middle layer, thick, smooth muscle and elastic
connective tissue c) tunica externa - fibrous connective tissue.
AORTA
- large lumen, thick walls, pulsatile blood flow, systolic=120 mmHg,
diastolic=80 mmHg
LARGE
ARTERIES- elastic reservoir to store part of the energy of cardiac contraction
MAIN ARTERY
BRANCHES/TERMINAL ARTERIES- to conduct blood to capillaries
ARTERIOLES- mainly smooth muscle,
affected by local and circulating substances (vasoconstrictor and vasodilator),
innervated by constrictor fibres mainly, main control of blood flow to organs,0.2-0.05mm
diameter, supply 10-100 capillaries,main resistance to blood flow.
METARTERIOLES-
smaller muscle-walled vessels, which feed into capillaries
Veins:Have
larger diameter and thinner walls than arteries, easily distended,have smooth
muscle, innervated by vasoconstrictor fibres, valves present in veins, except
for smallest veins, venae cavae, veins from brain, portal system and pulmonary
veins.
Blood
reservoir- 55% of blood in systemic veins, 12% in heart, 18% in pulmonary
circulation.
VENULES-
0.02-0.05mm diameter, outside layer of smooth muscle,controls outflow of blood
from capillary bed
TERMINAL
VEINS->MAIN VENOUS BRANCHES-->LARGE VEINS-->VENA CAVA (3 mmHg
pressure, conduct blood back to heart)-->RIGHT ATRIUM
Physical
factors affecting movement of blood:
Flow (volume/time) of blood is directly
proportional to pressure and inversely proportional to resistance. Flow can be
silent (no sound) or turbulent (noisy).
Flow= (Pπr^4)/(8η1) i am not sure about the equation please check this
Resistance:
The
resistance to blood flow is affected by the length of vessels, the radius of
vessels and the viscosity of blood. Changes of radius are the most critical in
determining resistance and hence flow of blood. Arterioles are major sites of
resistance
Viscosity:
Blood
is 3-4 times as viscous as water. Plasma is 1.8 times as viscous as water.
Viscosity in vivo is less than in vitro. An increase in the cellular
composition of blood i.e haematocrit, increases viscosity , whilst anaemia
leads to a decrease in viscosity. An increase in temperature leads to a
decrease in viscosity and thus a decrease in resistance, whilst a decrease in
temperature leads to an increase in viscosity. Increased viscosity will lead to
increase work for the heart and thus possibly heart failure.
Opening
and closing of blood vessels:
The
pressure inside blood vessels (distending pressure-P) must be balanced by the
tension (T) on the outside walls of the blood vessels caused by the weight of
tissues to prevent collapse or rupture. This is described by the law of Laplace (P=T/r, where r= radius). The smaller the radius,
the lower T has to be to balance P. Thus capillaries despite their small size,
don't rupture.
The
microcirculation
capillaries, lymphatics, Starlings law, exchange of fluid, oedema
Consists
of the capillaries and Lymphatic vessels.
The microcirculation has a large cross sectional area, thus low blood
flow, its walls are very permeable and is adapted for exchange of water, gases,
nutrients and waste materials.
Capillaries:
Are short narrow tubes (10 billion
capillaries, surface area= 500 m2, one cell thick (1mm), up
to 1mm long diameter= 7-10 um), which have a wall made up of a single layer of endothelial
cells plus a basement membrane. They do not have smooth muscle. Within the
walls are slit like pores (50-90x10-9 m. The capillaries in
different parts of the body vary in their leakiness. Three main types can be
distinguished i) Continous - found in nerve, skeletal muscle, fat and skin with
very few pores ii)Fenestrated - found in intestines, endocrine organs and
kidney these have small gaps iii) Discontinuous - found in liver, spleen and
marrow, which have large intercellular gaps.
In
areas such as the skin, ears and fingers there are shunts (Arteriovenous
anastomoses), which are direct channels between the arterioles and venules, and
are under nervous control (mainly constrictor fibres). Blood flow controlled by
precapillary sphincters (minute bands of smooth muscle) and arterioles.
The
function of the capillaries is exchange of substances. This is brought about by
filtration, absorption and diffusion. These are determined by the leakiness of
the walls, the capillary pressure and osmotic pressures according to the
Starling model. Starling (1896) formulated the principles governing the
exchange of fluid across capillaries. Three main factors were involved:
1/
Hydrostatic pressures- these are forces which tend to push fluid e.g. capillary
blood pressure, interstitial (outside cells) fluid hydrostatic pressure
2/
Osmotic pressures- forces which oppose the pushing tendency of the hydrostatic
pressures and are mainly caused by proteins e.g. capillary osmotic
pressure and interstitial hydrostatic
pressure
3/ The
conductivity of the capillary wall- the rate of transport of fluid across the
capillary wall, which is affected by the area, distance across the capillary
wall and viscosity of the fluid. Permeability varies e.g. very permeable in
liver, spleen and bone marrow whilst practically impermeable in skeletal muscle
Both
hydrostatic and osmotic pressures are on both sides of the capillary membrane,
thus it is the difference in pressure across the capillary wall membrane which
is important in exchange of fluid. If we consider the arterial end of the
capillary, here the higher hydrostatic pressures favour filtration i.e. fluid
leaks out into the tissue spaces. In the venule end of the capillary, the
higher osmotic forces favour absorption from the tissue spaces i.e fluid leaks
back into capillary. The balance of filtration and absorption may vary with
changes in arterial tone. Capillary pressures on average are between 20-30
mmHg, however these pressures can vary widely depending on location e.g.s the
glomeruli of the kidney= 60-70 mmHg; pulmonary capillaries= 7 mmHg.
Lymphatic
system:
Is
closely associated with the circulation, and are a series of thin walled
vessels with valves that provided an alternative route for return of
interstitial fluid, proteins, and fats via thoracic duct to venous system. The
fluid that is returned is called LYMPH. Lymph nodes within the system filters
lymph in removing bacteria and viruses. It has many valves and smooth muscle,
and the fluid is propelled by external compression on lymph vessels by
contracting muscles.
Lymphatic vessels:
Are
porous, thin walled vessels resembling capillaries in all tissues except bone
and central nervous system. Their function is to clear the interstitial spaces
of excess fluid, proteins, lipids and foreign materials and return it to the
vascular system. They are different from the capillaries in that their walls
are attached to surrounding tissues thus preventing collapse and they are
designed for entry of fluid. Large lymphatic vessels have muscular walls. The
fluid that is carried in the lymph vessels is called Lymph, with a composition
similar to plasma but with very little protein. The flow of this fluid is slow
(2-4 L/day). The return of this fluid is made easier by compressing lymph
vessels, by skeletal muscle contractions and by the presence of one way valves.
Oedema:
Is the
accumulation of excess fluid in the interstitial (tissue) spaces of the body
e.g. in feet, around eyes. It can be caused by 3 main factors
i)Hypoproteinaemia- low plasma protein in capillary, thus greater outflow of
fluid into the tissue spaces ii) Increased venous pressure, thus an increase in
filtration from capillary and thus an increase in fluid in the interstitial
spaces iii) Lymphatic obstruction- thus protein leaks from capillary lack of
reabsorption of fluid.
Lecture 2. The cardiac cycle:
Definition of one cycle. Its
importance. Electrical aspects of one cardiac cycle, pacemaker potentials and
non-pacemaker potentials, the conductive tree and the ECG. Practical
measurement of an ECG and its importance. Dysfunction: Arrythmias and heart
abnormalities. Mechanical aspects of one cardiac cycle. Sounds and pressure
changes in the aorta and left ventricle and their importance to blood pressure
and cardiac output. Dysfunction: Heart failure.
The
heart pumps blood for approx. 70 years. It has a weight of 300g for a man of 70
kg weight. The heart rate is 65 to 80 in resting man. At each heart beat 70-80
mls of blood is ejected into the aorta, known as the stroke volume.
The
Cardiac Cycle
is the
period (0.8 s) from one heart contraction to the next, started by the action
potential from the sino-atrial node. It consists of 2 parts, diastole (period
of relaxation- 0.5 s) and systole (period of contraction- 0.3 s).
The
importance of the cycle is twofold. 1/ It maintains blood flow for all the
organs in the lifetime of the individual and 2/ Supplies the blood pressure to
maintain the circulation.
Electrical events of the cardiac cycle:
To
understand the mechanisms underlying contraction of cardiac, skeletal and
smooth muscle we need to examine the structure and forces across cell
membranes, particularly the membranes of nerves and muscles. In the 18th
Century, it was noticed by the Italian, Galvani, that frog's legs twitched when
they were hung on metal railings in a thunderstorm. But it was not until the
1940s and 1950s that the mechanisms underlying this twitching were elucidated.
Hodgkin et al, using isolated Squid axons (large in size, easy to manipulate
their structure), manipulated the concentrations of ions inside the axon and
measured movement of these ions across the membrane (using radioactive
isotopes). They found that the inside of the axon had a negative potential to
the outside, there was mainly potassium inside and mainly sodium outside, and
that nerve transport occurred when sodium entered the inside and set up a
depolarising current (action potentials). Hodgkin and Huxley (1949), developed
a technique called the 'Voltage Clamp Method' (a feedback method to hold
membrane potential) to investigate the changes in membrane potential as nerve
transport occurred.
The next major advance occurred in the 1960s
when chemicals were found to block action potentials. Tetrodotoxin (TTX) found
in the 'Puffer fish' blocks sodium channels and causes paralysis and death.
Tetraethylammonium (TEA) blocks the potassium channels. Both these blockers
allow investigation of these channels.
Neher and Sackman (1970s) developed a novel
technique('Patch Clamp), by which individual ionic channels could be studied.
Very fine glass micropipettes (diameter=um) literally grasps a single channel
and measures the current flow through the channel. These channels conduct ions,
they are selective, they function like gates or switches and thus control flow,
they are differrent types of proteins. For example, the sodium channel is a
single protein molecule (composed of 1800 amino acids) folded into 4 parts (but
precise shape unknown), it is selective to only sodium and is voltage gated
(opens or closes depending on the voltage).
Resting Potentials:
These
vary depending on the type of tissue (e.g. muscle membrane=-90mV, blood cell
membrane=-9mV). The value depends mainly on the concentration of sodium and
potassium across membrane (Na+ outside = 145 mM; Na+ inside = 10 mM; K+ outside
= 4 mM; K+ inside= 135 mM). However, the chloride ion (Cl-) also contributes.
The concentration differences and the charges carried by the ions lead to
chemical and electrical forces across the membrane. For each ion, the
contributions these forces make to the resting potential can be calculated by
using the Nernst equation (e.g. Ek=61.5 log10 [Ko+]/[Ki+]
at 37C, where Ek represents the voltage due to potassium ions,Ko+
and Ki+ are the concentrations of potassium inside and
outside the membrane). Another equation which may be useful is the Goldman
equation. The latter gives the size of the membrane potential at any given time
for all the ions. The other determinants of the resting potential are the
membrane permeability, and the active Na+/K+ ATPase (sodium-potassium pump) which
pumps sodium out and potassium in.
Cardiac Muscle:
The
cardiac muscle (myocardium) is striated (like skeletal muscle), muscle fibres
consist of the proteins actin (thin, MW=42,000) and myosin (thick, MW=480,000).
Cardiac muscle is a syncytium, i.e. the cardiac muscle cells are tightly bound
together (actually there are 2 syncytiums, one for atria and the other for the
ventricles). Each cell is 50-100 um long and 10-20 um wide. Between the cardiac
muscle cells are intercalated discs (within which are gap junctions) which
provide low electrical resistance and thus allow fast diffusion of ions and
thus electrical activity. Skeletal muscle cells are isolated due to lack of
these gaps. Stimulation of any single muscle fibre causes the electrical activity
to travel over entire heart muscle. Cardiac muscle has the property of
autorhythmicity, i.e. an external stimulus is not required to activate the
cardiac cells. There is a delay of 10 ms for cardiac muscle between electrical
activity and contraction (in skeletal muscle the delay is 2 ms). Cardiac muscle
cannot be tetanised unlike skeletal muscle, nor can it fatigue.
The
electric potential within a cardiac fibre is due to a semi-permeable membrane
and the ionic composition inside and outside a cell. A value of -70 to -90 mV
is commonly found. Resting potentials at the Sino Atrial node are lower (-40
mV).
The
action potentials produced by depolarization (due to Na+ ions moving
into cell), leads to release of Ca2+ ions which lead to contraction
of cardiac muscle, followed by repolarization (K+ ions moving into
cell). The time course of this depolarization and repolarisation varies
depending on the part of the heart.
Contraction
of cardiac muscle occurs with myosin and actin forming crossbridges (sliding
filament theory) in the presence of calcium. Relaxation is an active process
(requires ATP) involving the rapid removal of calcium by ATPase and Cyclic AMP.
Conductive tree:
The
action potential originates at the Sino-Atrial (SA) node (located at the
junction of the Superior Vena Cava and the Right Atrium), travels across the
atrial muscle, to the Atrio-Ventricular (AV) node (takes 66 ms), the Bundle of
His (130 ms), then the right and left branches of the Purkinje fibres (260 ms).
Speed is fastest in the purkinje system (5 m/s). The conduction through the AV
node is slow (0.03-0.05 m/s) compared to atrial or ventricular muscle, to
ensure that atrial contraction is completed before ventricular contraction
begins.
Cardiac action potentials:
The
shape and durations of the action potentials generated along the conductive
tree varies, but they can be grouped into two major types, pacemaker and non-pacemaker.
1/ Pacemaker:
These
include those produced at the SA and AV nodes. Durations vary between 200-250
ms. The action potentials here are slow. The resting potential of these areas
are between -40 to -60 mV, they are slowly depolarising constantly (upstroke
due to combination of fall in K+ current, and rise in Ca2+
and Na+ currents) with very litle resting period, there is no
plateau in the shape, and there is also a slow repolarisation (potassium
currents). The pacemakers vary their discharge by 3 mechanisms, namely change
in slope of depolarisation, changes in threshold potential for starting the
action potential and the absolute value of the resting potential. The discharge
rate is altered mainly by the autonomic nervous system (parasympathetic and
sympathetic nerves) and circulating adrenaline. Parasympathetic nerves release
Acetylcholine which slows the heart rate, whilst Sympathetic nerves release
Noradrenaline which increases the heart rate. Adrenaline released from the
adrenal medulla also increases the heart rate and force of contraction.
2/ Non-Pacemaker:
These
are found in the atrial muscle, ventricular muscle (durations=250-300 ms) and
the purkinje fibres (300-400 ms). The action potentials here are fast. The
resting potentials here are much larger (-90 mV), there is a very rapid
depolarisation (upstroke - due to rise in Na+ and fall in K+
currents); a rapid but short decline due to inactivation of fast Na+
current; a plateau (due to Ca2+ mainly and and slow rise in Na+),
and a repolarisation (due to K+,Ca2+ and Na+
currents). The shape shows a plateau, which allows action potential to last
10-30 times longer than in skeletal muscle, and thus increases the period of
contraction. The reason for the plateau is a) large store of calcium and
calcium influx continuous for 0.2 to 0.3 seconds i.e is prolonged b)
immediately after start of action potential, there is a 5 fold decrease in
potassium permeability of cardiac muscle membrane for 0.2-0.3 s which prevents
repolarization of the membrane and thus contributes to plateau.
There
is an absolute refractory period (200 ms) during which another action potential
cannnot excite the cardiac cell. This is very important in allowing the
ventricles to relax and refill with blood.
Measurement
of E.C.G.:
Principle: As
the action potential spreads across the heart and across the body, it can be
viewed at any instant as an electric dipole (depolarised part being negative
whilst polarised part is positive). An electrode placed on the skin can measure
the change in potential produced by this advancing dipole. This forms the basis
of the electrocardiogram or E.C.G.(a record of the electrical activity
generated by the heart).
The
E.C.G. can be recorded by measuring the potential difference between any two
points on the body. These two points when taken together constitute a LEAD. The
potential difference measured by the lead depends on the size of the electric
dipole (wave of electrical depolarization), the direction of the electrodes and
the distance of the electrodes from the dipole. The E.C.G. is normally recorded
at a paper speed = 25mm/s and a gain or vertical deflection of 1 mV=10 mm. A
full E.C.G. recording is made up of 12 leads. 6 leads record the electrical
activity in the vertical plane (head to foot), whilst the other 6 leads
(chest), record in the horizontal plane (across the chest).
Einthoven
in 1903 developed the first practical device for recording cardiac potentials,
called the string galvanometer, which became the Electrocardiograph. He
developed the classical limb lead system, whereby an electrode is placed at
each corner of an imaginary equalateral triangle superimposed on the front of a
person (known as Einthoven's triangle). The three corners represented right arm
(RA), left arm (LA) and left leg (LL).
Lead I
was a recording of the cardiac potentials between RA and LA.
Lead
II = recording between RA and LL.
Lead
III = recording between LA and LL.
Einthoven's
law- Lead I + Lead III = Lead II
Wilson in
1934, developed a further system, which amplified the action potentials, known
as the Augmented (a) lead system (leads 4,5 and 6) called aVr (right arm), aVl
(left arm) and aVf (foot).
Components of the E.C.G. trace:
P wave:
atrial depolarisation, duration=0.1 s, height=< 2.5mm or 0.2mV
P-R interval: conduction time over
the atria and ventricles, time from beginning of P to beginning of QRS complex, usually 0.12 - 0.16 s.
QRS complex: depolarisation of
ventricles, duration= lead II is
0.08-0.12s and 1mV not>35 mm
ST segment: is a straight line at
end of ventricular depolarisation. From end of S wave to beginning of T wave.
Here heart is depolarized, hence isoelectric, duration= 0.08s.
T
wave: ventricular repolarisation, normally positive i.e.
upwards, 0.16-0.27s and 0.2-0.3mV.
QT
interval: time from the beginning of the QRS to the end of the T
wave, 0.3-0.34s;
PR segment: time from end of P wave to
beginning of QRS complex, 0.03-0.06s; impulse travelling through AV node, AV
bundle and Purkinje fibres, no change in surface potential, hence isoelectric.
Heart
rate = count the number of QRS complexes. Atrial repolarisation hidden by QRS
complex.
Clinical
Aspects: E.C.G. can be used to detect disturbances in initiation
and propagation of action potentials (cardiac arrythmias), e.g. in Ischaemic
Heart Disease. Another cause of disturbances would be generation of latent
pacemakers (ectopic foci) along the conductive tree.The electrical axis gives
the overall direction and size of the electrical impulses conducted over the
heart, it is normally 59 degrees. It indicates the approx. position of heart in
thoracic cavity and possible hypertrophy of heart chambers, i.e <0 degrees=
left axis deviation, if >90 degrees= right axis deviation.
Arrythmias
Are heart rhythm abnormalities. There are 2 main causes,
extra excitatory signals or malfunction of conductive system.
1. Heart
block: 3 types- i) 1st degree =incomplete heart block, very slow AVN conduction
ii) 2nd degree = only a fraction of normal conduction iii) 3rd degree = no
conduction between atria and ventricles eg. Ischaemic damage to AVN or bundle
of His. This may lead to new pacemakers
(ectopic foci) in purkinje or bundle of
his.
2. I)
congenital conduction pathways eg. Extra pathway between atrial muscle and AVN
thus Increase in heart rate to 150b/min-250b/min, problem caused by re-entry or
recycling of impulse; there could also be a separate pathway between atria and
ventricles causing again re-entry problems. II) Extra post depolarisations or
extra depolarisations before repolarisation is complete due to increased Ca2+
current.
3. Hypoxia-
causes Ischaemia, which increases the K+ channels to open, thus shortens action
potential and thus reduces contraction.
4. Hyperkalaemia-
increased K+ in plasma, causes cell membrane to depolarize, thus arrythmias and
fibrillation
Treatments : ca2+ , K+ , Na+ channel blockers and beta
blockers
Mechanical
events of the cardiac cycle:
Figure (1) shows some of the mechanical
events in one cardiac cycle for the left side of the heart. This includes the
E.C.G., 2 heart sounds, pressure changes in the aorta and left ventricle and
blood volume change in the left ventricle.
One cardiac cycle is described below from one P
wave to the next P wave.
The P
wave signals electrical excitation of the atria, spreads over atrial muscle,
atrial contraction starts, thus slight increase in atrial pressures, and blood
pumped into ventricles (0.16 s), excitation spreads over ventricles, QRS
complex starts, ventricular contraction begins, thus increase in ventricular
pressures, closes the atria-ventricular valves thus causing the first heart
sound (Lubb), ventricles now become a closed chamber since the semilunar valves
are already closed, ventricular pressures increase rapidly (isovolumetric
contraction), exceeding the pressures in the pulmonary artery and aorta, thus
opening the semi-lunar valves, ejection of blood from ventricles occurs (rapid
phase followed by slower phase), ventricular relaxation (pressures drop,
closing the aortic and pulmonary valves- thus 2nd heart sound- Dubb), at end of
ventricular relaxation the atria ventricular valves open because ventricular
pressures become less than atrial pressures, a phase of rapid filling of
ventricles (0.1 s) followed by a phase of slow filling (0.2 s) occurs which is
finally ended by the atrial systole.
Important
features of the mechanical events:
Heart Sounds:
There
are four heart sounds, two of which can be heard clearly on surface of chest
with stethoscope. First is 'Lubb'
has a f= 30-45 Hz,duration= 0.05 s, caused by AV valves closing and vibrations
in cardiac muscle. Second is 'Dubb'
occurs at end of T wave, with f= 50-70 Hz, duration= 0.025 s, caused by closure
of semilunar valves. Abnormal heart sounds are called 'murmers', and can occur
due to narrowing or increased resistance of pathways (e.g. valves) to blood
circulation.
Aortic pressure wave:
Rising
part is synonymous with pressure rise in ventricle. Highest pressure is the
systolic pressure. Dicrotic notch is due to temporary backflow of blood from
aorta into left ventricle, this backflow stops with closure of aortic valve,
producing sharp recoil of walls of aorta, peripheral flow of blood continues
due to elastic recoil of the arterial walls. Resting level is the diastolic
pressure.
Left Ventricular Pressure Wave:-
Shows 4 parts (1, 2, 3, 4)
Both
rising(2) and falling parts(4) are the same shape. Rising part (Isovolumetric
contraction) gives an indication of the strength of the heart, and determines
systolic pressure and also the cardiac output. This is the most important
waveform in terms of generating enough pressure and blood flow for the body.
Notice the low starting and high finishing pressures of the waveform.
Left Ventricular Volume:
When
the bicuspid valve is closed, the amount of blood accumulated in the left
ventricle at the end of diastole is known as the End diastolic volume. When the
semilunar valve is closed, the amount of blood left in the left ventricle is
known as the End systolic volume.
Lecture 3. Blood Pressure:
Definition of blood pressure. Its
importance and regulation. Short term regulation by hormones and baroreflex
mechanism. Long term regulation by kidney and blood volume alterations.
Measurement of blood pressure. Dysfunction: Hypertension and its importance to
other diseases eg coronary heart disease, stroke.
Stephen
Hales (1677-1761) - a clergyman, was the first to measure blood pressure in a
horse. Claude Bernard (1813-1878) showed in 1851, that the sympathetic
discharge to the blood vessels was excitatory (vasoconstrictor tone). Karl
Ludwig (1816-1895) in 1847 invented the kymograph and made the first continous
recording of blood pressure. Rene Laennec (1781-1826) invented the stethoscope.
In
1733, Stephen Hales (1677-1761, pastor, physiologist, botanist) connected a
cannula or fine tube to a glass tube held vertically from the carotid artery of
a mare, and found that the blood rose to 3m, and suggested connection between
blood pressure and atmospheric pressure. This discovery had no effect on
medicine for the next 150 yrs. He was also the first person to correctly
measure the capacity of the LV,
and to measure cardiac output per minute, the speed of the blood flow in the
vessels. In 1876 Von Basch produced the first apparatus to measure blood
pressure without cutting an artery, but it was complicated to use (despite
modification by the Italian Riva-Rocci in 1896), but the principle was
accepted, that of an inflatable tourniquet to which a manometer was attached.
The method was refined by the russian surgeon Korotkoff in 1905, by applying
stethoscope to pulse area.
Arterial
blood pressure varies with age, sex, metabolic rate, emotional state, sleep,
postural changes and other factors. Normal values are expressed as a range.
e.g. age 20-24, male systolic= 105-140, female systolic=100-130, male
diastolic= 62-88, female diastolic=60-85. Arterial blood pressure increases
with age, with pressures of women being 5-10 mmHg lower on average until the
age of 50, after which pressures don't differ. An individuals blood pressure is
normally expressed as systolic/diastolic. Hypertension is quoted as 165/95 and
above. Moderate hypertension is 140/95.
Maintanance of an adequate blood supply to the brain,
heart and kidney is intimately dependant on the level of the general arterial
pressure (mean arterial pressure- M.A.P.). The M.A.P. is the average pressure
during the cardiac cycle. M.A.P. is
also equal to = Diastolic pressure +
1/3(pulse pressure)
|
The
M.A.P. is the result of discharge of volume of blood from the heart to the
arterial system, which cannot all escape through to the venous system before
the next beat occurs. This means i) the arterial system is overfilled and ii)
elastic arterial walls are stretched. Thus M.A.P is dependant on the cardiac
output (C.O.) and the total peripheral resistance (T.P.R.). Thus factors
affecting C.O. (the output of blood from the left side of the heart) and T.P.R.
(the total resistance offered by the vessels to blood flow) will determine the
value of M.A.P.
The
systolic ejection of blood from the left ventricle to the aorta, creates a
pressure waveform (arterial pulse wave) in the aorta and is transmitted to the
rest of the arterial tree (refer to the aortic pressure waveform on handout).
This waveform is asymmetrical. The peak of this waveform is the systolic
pressure (120 mmHg) and the base (when heart is relaxing) is the diastolic
pressure (80 mmHg). M.A.P.(approx. 100 mmHg) is the average effective pressure
forcing blood through the circulatory system and is midway between these two
pressures. Arterial pressure is pulsatile during each cardiac cycle. The pulse
pressure which can be felt readily on the radial and carotid arteries, is the
difference between the systolic and diastolic pressures. The blood pressure
within an artery varies during each cardiac cycle and hence the arterial pulse
wave varies. The size and shape of the arterial pulse wave are directly related
to the stroke volume and inversely related to the compliance (elasticity) of
the arterial vessels. The speed of this wave is slow in the large arteries
(3-5m/s)
and
faster in the small arteries (14-15m/s) and this also relates to elasticity.
Factors affecting blood pressure:
1/ C.O. = stroke volume x heart rate
2/
Starling effect- increased stretching of heart muscle leads to increased
contraction.
3/
Sympathetic stimulation- causes an increase in heart rate, and in force of
contraction.
4/
Parasympathetic stimulation- mainly decreases the heart rate and slight
decrease in force.
5/
Peripheral resistance- particularly of the arterioles.
Sympathetic nerves are extremely important in regulating blood pressure and
thus blood flow.If these arteriole vessels constrict, then the outflow to the
veins is temporarily reduced and thus M.A.P. is increased, whilst if vessels
dilate, M.A.P. is decreased. Variations in the diameter of the arterioles of
the abdominal (splanchnic) region are more effective than other areas in
causing changes in M.A.P. The splanchnic vessels when fully dilated have an immense
capacity to hold blood volume. Sudden strong emotion may cause their dilation,
and thus a fall in M.A.P. and may lead to fainting.
6/
Blood volume- a sufficient amount is required to overfill the arterial system.
Haemorrhage causes a decrease in blood volume and thus M.A.P. falls. Atrial
Natriuretic Peptide (ANP or ANF), released from the atria due to stretching of
atria, can decrease blood volume in minutes, by action on the kidney to
increase water loss, decrease sodium reabsorption, and also decrease release of
ADH and renin/aldosterone. It also causes vasodilation of arteries and veins.
Blood volume can be increased by the hormones renin, angiotensin II,
aldosterone and ADH, which can thus raise blood pressure.
7/
Viscosity- Blood is 5 times more viscous than water. Thus increased viscosity
causes an increase in resistance to blood flow and thus increased work for the
heart.
8/
Elasticity of the arterial walls- elasticity (and thus the recoil of the vessel
walls) and the peripheral resistance ( to prevent escape of too much blood to
the venous system) are essential for the development of the diastolic pressure.
Control
of blood pressure:
This
can be split into short term (minutes, hours- e.gs posture, acute stresses,
haemorrhage) to long term (days, weeks- e.gs blood volume, hypertension).
Short Term control:
Baroreceptor reflex:
(negative feedback control).
This
reflex maintains short term control 60% of the time. High pressure receptors
called arterial Baroreceptors (nerve endings in vessel walls) are found in the
arch of the aorta and the carotid sinus, and they respond to stretch. They
monitor the pressure of the blood comming from the aorta and carotid artery
respectively. They have two reflexes affecting the heart and thus cardiac
output and the blood vessels and thus the peripheral resistance.
Consider a rise in blood pressure in the body:
This
will cause an increased discharge from the baroreceptors via the vagus and
glossopharyngeal nerves to the cardivascular control centres (cardiac and vasomotor
area in the medulla- excitatory and inhibitory areas) in the brain. This leads
to an increased discharge of parasympathetic nerves to the heart and a
decreased discharge of the sympathetic nerves to the heart, with the effect of
decreasing the heart rate and stroke volume. There is also a decreased
discharge down the sympathetic nerves to the arterioles, producing vasodilation
and thus a decrease in peripheral resistance and the net overall effect is to
return blood pressure to normal. The reverse of these changes take place for a
fall in blood pressure in the body.
Certain
situations the baroreflex may be suspended temporarily, e.gs. i) during
exercise- increase in systolic pressure during exercise ii) diving (face
immersion) reflex- sharp decrease in both heart rate and arterial pressure iii)
stress- increase in blood pressure.
Cardiopulmonary
reflexes:
There
are a variety of other receptors which sense low pressures, mainly in the walls
of the heart (atria, ventricles), pulmonary vessels and vena cava which
supplement and modulate the baroreceptor reflexes. These receptors are mainly
affected by stretch. The resulting reflexes are involved in both short term and
long term control. e.g. increased stretch of the atrium, releases ANF, which
affects the kidney to alter the blood volume. A decrease in atrial receptor
stimulation can increase blood volume. Both inhibitory (e.g. bradycardia,
vasodilation and inhibition of breathing) and excitatory responses can be
produced from receptors in the ventricles mediated by vagal and sympathetic
nerves and local metabolites (e.g. prostaglandins, serotonin, bradykinin).
Long
term control: Involves
regulation of the normal blood volume of 5.5 litres. This means regulation of
the plasma volume (PV) and the red cell volume (RCV). RCV is determined by the
number of red blood cells, thus bone marrow and erythropoietin and changes take
place more slowly in days and weeks. PV is affected by both fluid input and
fluid loss and thus more rapid changes. The main factor in regulation is the
kidney, which regulates the water and sodium content. Sodium is extremely
important to maintaining the plasma volume. Factors which affect the blood
volume include:
i)
Vasopressin (ADH)- released from the posterior pituitary and decreases water
loss and thus sodium reabsorption ii) Renin-angiotensin-aldosterone system - If
renal arterial pressure is low, or low sodium chloride, or increased renal
sympathetic activity leads to secretion of the hormone renin, which breaks the
plasma protein angiotensinogen into angiotensin I and then angiotensin II. The
latter is a powerful vasoconstrictor (half life 30s), and also increases sodium
reabsorption by proximal tubule, and stimulates the release of aldosterone (and
cortisol) from adrenal cortex, which reabsorbs sodium and also stimulates ADH
release. iii)Atrial Natriuretic Peptide (ANP)- Is a 28 amino acid released from
the atria by large atrial stretch, which produces diuretic responses from
kidney, also vasodilation and decrease in renin release. IV) Renal efferent
nerves (sympathetic fibres)- increased activity leads to direct sodium
reabsorption by proximal tubule and activation of ii) and thus increase in plasma volume. v)
Factors which affect venous capacitance can affect distribution of blood within
the body.
A
variety of drugs are used to decrease high blood pressure (hypertension). These
drugs bring about their effects by i) vasodilation - e.g. Hydralazine ii)
Smooth muscle tension decrease calcium channel blockers e.g. Nifedipine iii)
changing blood volume - diuretics e.g Thiazides iv) Angiotensin Converting
enzyme inhibitor- e.g. Captopril v) reducing the cardiac output of the heart -
reducing the sympathetic effects on the heart e.g. Propranolol
Measurement
of Blood Pressure:
A
direct invasive measure can be obtained from radial artery puncture and
connecting needle and catheter to a pressure transducer. Riva Rocci first
suggested an indirect measure of blood pressure. The most common non-invasive
procedure is the method of Auscultation (sounds) developed by a Russian surgeon
called Korotkoff in 1905. The apparatus involves a Stethoscope to listen to
sounds and a sphygmomanometer consisting of an inflatable cuff (Riva-Rocci), a
mercury manometer to measure pressure, a small rubber handpump with valve to
increase or decrease pressure. Subjects sit on a comfortable chair with either
their left or right arm resting on a flat surface. After removal of any
restraining clothes, a cuff of appropriate size is wrapped around the upper
arm. The cuff is inflated to a pressure of 150-160 mmHg. After placing the
stethoscope drum on the Brachial artery, the pressure in the cuff is released
gradually, after a while sounds can be heard (Korotkoff sounds) until the first
heart sound is heard (this is the systolic pressure), pressure drop is allowed
to continue when further sounds can be heard. The dissapearance of the last
sound determines the diastolic pressure.
Demands
on the Cardiovascular System
AIMS
1. Exercise,
Stress, shock
2. CHD and
Hypertension?
3.
Treatments for CVD?
EXERCISE
- Definition: A single bout of bodily exertion or muscular activity that requires energy expenditure above resting level, resulting usually in voluntary movement.
- Description: Intensity (maximal or submaximal);duration; type
- Aerobic (dynamic, isotonic)
- Non-aerobic ( isometric, static) Isokinetic
Successful exercise
•
muscular,
CVS, respiratory
•
Adequate
gas exchange- O2 & CO2
•
Availability
of fuel- glycogen, glucose, fatty acids
STEPS IN EXERCISE
3 STAGES
- 1. Anticipation- preparatory, HR, C.O.
- 2. During- main changes- metabolic, respiratory,CVS, blood flow redistribution
- 3. Recovery- return to resting conditions, payback of O2 debt, metabolic replenishment
Physiological changes
CVS
INCREASE:
•
blood
flow to muscles
•
1 to 22-33 l.min-1
•
SNS, A, NA
•
metabolic hyperaemia
•
indirect PNS

-
SP, DP, C.O. SV, HR

- Respiratory
–
VE,
Pulmonary blood flow, bronchial dilation, VO2
–
O2
, CO2, anaerobic metabolism, pH, RQ
–
O2
extraction- intensity, capillary density, Bohr shift to right, aerobic enzyme
activity

Limitations to exercise
- Healthy
–
gas
exchange-delivery/extraction of O2,removal of CO2; maximal cardiac output
–
availability
of fuel/metabolic capacity of active muscle
–
controlling
body core temperature
–
muscle
fatigue
–
increase
in lactate
- Disease
- Jones & Killian (2000). Exercise limitations in health and disease- NEJM 343(9):632-641
–
Pain,
dyspnoea, increase in perceived effort
–
reduced
aerobic and ventilatory capacities
–
muscle
weakness
What
is shock?
‘Acute
circulatory failure
-general
cellular hypoxia
-inadequate tissue perfusion’
CAUSES?
- Inadequate blood flow to vital organs
Symptoms
- low C.O.
- low B.P.
- pale, grey
- rapid shallow breathing
- rapid weak pulse
- decreased urine
Types of
shock?
w Hypovolaemic
w Cardiogenic
w Mechanical
w Septic
w Anaphylactic
Cardiovascular
Disease
- CAD [ CHD, IHD, ]
–
Ischaemia, atherosclerosis, arrythmias,
thrombosis, angina, MI,
–
major cause of death in western world
–
Hypertension, Heart failure, Valve disease,
cardiomyopathies, congenital, Tachyarrythmias and Bradyarrythmias, cardiac
infections, pulmonary embolism, MI, Hyperlipidaemia, aortic dissection,CHD
PRIMARY
RISK FACTORS
- SMOKING
–
4000 chemicals- diseases of lungs, heart, blood
vessels, cancer
–
risk µ
no. Of cigarettes
–
Nicotine- addictive, increased A + NA, fatty acids, stickiness of platelets,
decrease fibrinolysis
–
CO- carbamino compounds, decreases ability of Hb
to transport O2, arrythmias
- HYPERLIPIDAEMIAS
–
lipids- fatty acids, cholesterol, lipoproteins,
chylomicrons, triglycerides
–
increased by diet, diabetes, ideopathic
–
risk µ [cholesterol]; risk µ LDL; risk µ 1/HDL
–
risk µ
1/ fish oils (w3, w6- FFA)
- HYPERTENSION
–
increase in SP, DP, TPR - increased workload
–
increase in blood volume e.g Na+
MECHANISMS
- Atherogenesis- plaque formation-(fatty streak, fibrous plaque, complex lesion)
- plaque= lipid rich core surrounded by fibrous cap, stable or unstable
- LIPIDS- increased amt deposited on intimal layer- complex plaques
- SMOOTH MUSCLE- no. Increased, secrete collagen and elastin to form complex plaques
- ENDOTHELIUM DYSFUNCTION
–
vascular tone
•
thromboxane A2, endothelin,
•
prostacyclin, NO
–
stickiness of lining
–
clot formation -increased fibrinogen
–
uptake of inflammatory cells
–
endothelial damage- free radicals
–
uptake of LDL and oxidized LDL
- complex plaques or ruptured plaques occlude lumen- angina, arrythmias, sudden death
HYPERTENSION
- 1 in 10 adults- high blood pressure
- 140/90, 160/95
- Age (>45)
- Gender (M>F)
- Major health problem
–
Strokes,
heart failure,
–
Major
risk factor- chd, dm
–
Renal
failure, tpr, lv hypertrophy
–
risk
µ pressure
- Basic cause unknown
–
2
types
–
Essential-
90-95%
–
Secondary-
5-10%
CAUSES
- kidney disease- renal artery stenosis
- obesity, alcohol, cushing’s syndrome, aldosteronism
- MAP= C.O. X T.P.R
- VASOCONSTRICTOR AGENTS
–
ANS-
increased SNS activity
–
A,
NA, angiotensin II, ADH, 5HT, PROSTAGLANDINS
- VASODILATOR AGENTS
–
KININS,
NO, ENDOTHELIAL DAMAGE, Ach
- IONIC IMBALANCE
–
Na+,
K+, Ca2+
- OBESITY
–
BMI,
WAIST/HIP RATIO
–
INCREASED
SV, C.O., SNS, PLASMA VOLUME, INSULIN, RENIN/ALDOSTERONE
- ALCOHOL
–
increased pressor effect, SNS, cortisol,
renin/angiotensin, sensitivity to
adrenaline
- INSULIN RESISTANCE- DIABETES
–
increased Na+, Ca2+, SNS
- family history, genetic, environment
- MISDIAGNOSIS
TREATMENTS
- AIMS
–
Pain,
O2 demand, workload
–
Quality
of life, mortality risk
- DRUGS
–
NITRATES,
b- BLOCKERS, Ca2+ antagonists, anticoagulents, lipid lowering
- SURGICAL
–
CABG,
PTCA, Revascularisation, left ventricular assist devices, heart transplants
- LIFESTYLE CHANGES
–
Diet,
weight control, exercise, stop smoking
DRUGS
- Nitrates- GTN, Isosorbide dinitrate
–
relieves
angina in minutes
–
vasodilator-
veins, arteries, coronary vasospasm, thrombosis, platelet aggregation
–
side
effects- headaches, B.P, HR
- Ca2+ antagonists- Nifedipine, Verapamil
–
relieves
angina - vasodilation of blood vessels
–
block
ca2+ channels- smooth muscle> cardiac
–
side
effects- headache, BP, peripheral oedema, AV node conduction block, force
- b- blockers- Propranolol
–
decreases
O2 demand, HR, SV
–
side
effects- -ve inotropy, C.O
- Anticoagulents- Aspirin, Heparin, LMW heparins, Hirudin,streptokinase, warfarin
–
decreases
clotting- suppresses platelet aggregation
–
inhibits
thrombin, clotting factors, increases prostacyclin, inhibits platelet receptors
- Analgesics- diamorphine, diuretics- thiazides, ACE inhibitors- Captopril, a-blockers- hydrallazine,
- lipid lowering- statins (simvastatin, fluvastatin), Niacin ( nicotinic acid), Resins (colestipol)
–
decrease
LDL, triglycerides, increase HDL
–
decrease
lipoprotein synthesis in liver
SURGICAL
- PTCA= percutaneous transcoronary angioplasty
–
less
invasive, faster recovery, cheaper, quick relief from symptoms
–
risk
of clot being dislodged, ischaemia, restenosis, long term improvement poor,
metal stents
- CABG = coronary artery bypass grafting
•
vessels
>70% stenosis- require grafts
•
long
saphenous vein, leg, 15cm needed, occlusion
•
Internal
mammary atery, chest, high reliability, long term usage, low occlusion rate
–
Operation
•
monitor
ECG, T, Blood, K+, clotting times
•
patient
anaesthetized, heparinised, chest exposed, heart connected to bypass machine, core temp= 26-28C
•
to
operate heart needs to be still (infuse cardioplegic solution), have little
blood (clamping aorta)
–
Disadvantages
•
invasive,
expensive, bleeding, poor cardiac output, arrythmias, post infection
–
Advantages
•
80%
of patients have complete relief, long term survival >10yrs
RESOURCES
Websites
Cardiovascular physiology online
Body fluids - somewhat good
Interactive Physiology Pearson
more resources will be added
Websites
Cardiovascular physiology online
Body fluids - somewhat good
Interactive Physiology Pearson
more resources will be added
Thank you for sharing such wonderful information! When it comes to health, there is nothing more important than managing to eat healthy food and doing exercise regularly.
ReplyDeleteHealth Jobs Australia
The cardiovascular system consists of the heart, blood vessels, and blood. The cardiovascular system serves several major functions that are necessary for life. Cardiovascular drugs manufacturer India manufactures medicines that increases the force of the heart's contractions, which can be beneficial in heart failure and for irregular heartbeats.Cardiovascular Drugs are Prescription drugs and medicines for diseases relating to the structure and function of the heart and blood vessels.
ReplyDeleteGood information for contract drug manufacturing organization
ReplyDelete