General Functions of the Respiratory System:
- Ventilation - moving air into and out of the lungs
- Gaseous exchange - replacing O2 and removing CO2 from the blood.
- Regulation of acid-base balance
- Air conditioning
- Speech/smell
- (Temperature and Fluid Balance)




The structure of the respiratory system:
- two lungs: covered by visceral pleural and connect to the inner thorax and diaphragm
- branching network of airways
- respiratory membrane
- supporting tissues
- ''separated'' into: conducting and respiratory exchange zones







 Zones of the respiratory system:
Zones of the respiratory system:
Conducting zone:
- trachea
- segmental bronchi
- bronchioles
- terminal bronchioles
Humidify, warm and filter the air to PROTECT
Respiratory exchange zone:
- respiratory bronchioles
- alveolar ducts
- alveoli
Create large surface area and thin barrier to AID DIFFUSION
Know the functions of the lungs and respiratory system and the anatomical and functional zones of the respiratory system
NOW! Lets talk about the following
- The thorax and respiratory muscles
- Mechanics of breathing
- Pressure changes in ventilation


Mechanics of Breathing video
What causes air to flow in bulk into and out of the lungs?
- Expiration: Diaphragm moves up
- Inspiration: Diaphragm moves down
Air Pressure Changes During Ventilation
Inspiration: P(atmosperic) > P(alveolar) = air moves into the lungs
Expiration: P(alveolar) > P(atmospheric) = air moves out of the lungs
Factors affecting lung mechanics
- Lung compliance - the distensibility of lung tissue
- Lung Elasticity - the ability to stretch and return to resting state
- Surfactant - produced by type II alveolar cells reduces surface tension in alveoli (caused by H2O) increases total lung compliance
- Airway resistance - air contact with walls of airways including narrowing of airways due to disease/infection etc like Asthma etc, This causes more energy to be required to deliver sufficient air
So to summarize the mechanics of breathing:
Inspiration: stimulus to diaphragm -> diaphragm contracts thorax expands -> pressure in lungs decreases Patm>Palv -> air flows in bulk from atmosphere to alveoli (from high pressure to low pres.)
Expiration: stimulus to diaphragm ends -> diaphragm relaxes and thorax mmoves inwards (passive) -> pressure in lungs increases Palv > Patm -> air flows in bulk from alveoli to atmosphere (from high to low pressure)
NOW! lets talk about:
- Lung volumes and ventilation rates
- Nervous control of ventilation
- Chemical control of ventilation
- Carbon dioxide (PCO2)
- Hydrogen Ions (H+)
 | |
| Wet Spirometry |


At rest
- Pulmonary ventilation rate (minute volume) =
respiratory rate (RR) x tidal volume (Vt) = 12Br/min x 500ml = 6000ml/min
- Alveolar ventilation rate = (tidal volume - dead space vol.) x RR = (500-150) x 12 = 4200ml/min
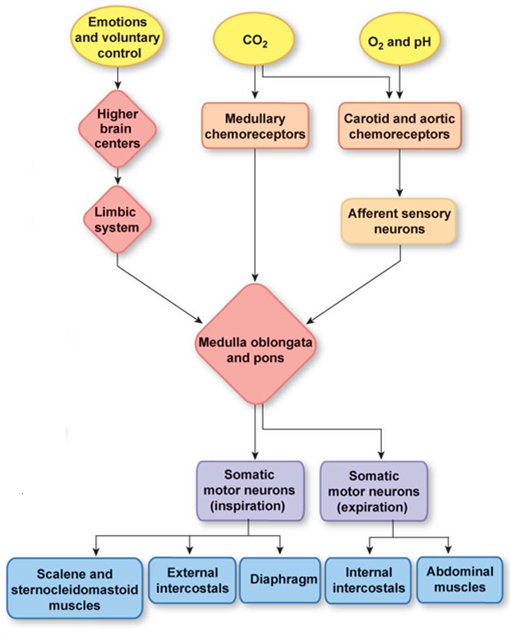
Regulation of Ventilation: Neural generation of rhythmic ventilation
- Ventilation depends on rhythmic on-off stimmulation of respiratory muscles via nerves
- automatic stimulus comes from the respiratory control centre in Medulla of the brain stem.
at the end of expiration => resting muscle tone neurones rhythmically 'fire' => active inspiration and then 'cease fire' => passive expiration

DRG sends an excitatory stimulus to the phrenic and intercostal nerve and the Pons
=> Phrenic and intercostal nerve conduct the stimulus to diaphragm and intercostal muscles - Active inspiration
=> Pneumotaxic centre in Pons sends an inhibitory stimulus back to the DRG and inspiration stops - Passive expiration

- PCO2 of arterial blood is the main input regulating ventilation under normal conditions
- Increased PCO2 stimulates ventilation via central and peripheral chemo-receptors
Central chemoreceptors
- Ventral surface of Medulla is sensitive to CO2-generated [H+] in cerebro-spinal fluid (CSF) surrounding medulla.
CO2 + H2O --> H2CO3 --> HCO3 + H+
- pH of CSF is more sensitive than blood as it contains fewer protein buffers
- Changes in PCO2 causes larger [H+] in CSF compared to blood.
Peripheral chemoreceptors
- carotid and aortic 'bodies'
- large blood supply
- both respond to PCO2 generated [H+] and blood pH
- Carotid also stimulated by decreased PO2
- PO2 only detected when it falls by ~40% (hypoxia/attitude)

Following topics about respiratory physiology to be discussed:
- partial pressure of gases
- O2 and CO2 transport in the blood
- ventilation and acid-base balance

Partial Pressure of gases
- Dalton's law: the total pressure of a gas mixture is equal to the sum of the pressures that each gas would exert independently when barometric pressure (Pb) is 760mmHg
The composition of atmospheric air is:
O2 20.93% 0.2093
CO2 00.03% 0.0003
N2 79.04% 0.7904
Calculation of partial pressures:
- the partial pressure of any gas can be calculated by multiplying Pb by the fraction of the gas
Example:
PO2 = 760x0.2093= ...mmHg
PN2= 760x0.7904= ...mmHg


 | |
| O2 transport by the blood |
........ arterial blood is fully saturated with O2.

 | |
| Oxy-haemoglobin dissociation curve |
This is described by the 'S' shaped. O2-Hb ..............curve. Each O2 molecule binding to Hb increases the rate of binding of the next O2 molecule
 |
| Effects of pH, temperature, PCO2 on O2-Hb |
Effects of pH and temperature on O2-Hb:
- Active tissues = ..............= increased [H+]
- Increased [H+] weakens the bond between O2 and Hb. More is released for a given PO2 when pH ......... O2-Hb dissociation curve shifts to the right called the ........
A similar shift to the right occurs with increased blood temperature around exercising skeletal muscle.

- CO2 diffuses into blood in systemic tissue capillaries. .......% remains dissolved in blood plasma. The rest (93%) diffuses into red blood cell (rbc). In rbc - ......binds to Hb = carbamino-Hb -.........% converted into H2CO3
- H2CO3 dissociates into HCO3- and H+
- HCO3- diffuses into plasma in exchange with .......
- H+ binds to buffers (Hb)
Ventilation and acid-base balance
- An increase in blood PCO2 leads to increased [H+] and this increases blood acidity (lower pH)
- A decrease in blood PCO2 has the opposite effect and the blood becomes more alkaline.
- Excessive ventilation will exhale more CO2 and reduce blood PCO2. Insufficient ventilation will result in a build-up of CO2 and increased blood PCO2.


Factors affecting lung mechanics
- Trans-mural pressure gradient
- Compliance, elastance, airway resistance, ST
 | |
| Lung Pressures |
- Intra-alveolar pressure (IAP) = Pb at rest -/+ ve 1mmHg midway through tidal breath
- Intra-pleural pressure (IPP) -4 to -8mHg <Pb (more -ve during inspiration)
- Transmural pressure gradient favours open airways (distending pressure)
Specific advantages of negative pump
Maintains:
- Alveoli patency
- Capillary patency
- Reservoir of air and blood
- Reduced fluid in alveoli
- Less energy needed to breathe
 | |
| Pathophysiology |
- Lung compliance
- Lung elasticity
- Airway resistance
- Alveolar surface tension forces
The cost of breathing
- 'Quiet' breathing = ~3-5% of total energy
- Energy and disease places higher demands (~30%)
- Compliance and airway resistance main contributors
Lung Compliance (Cl)
- Cl defines distensibility of lung tissue
- Cl the change in lung volume (Vl change) with a unit change in IAP (P change)
- The more the lung expands for a given rise in pressure the greater the Cl
Lung elasticity
- Provided by fibro-elastic network
- Allows passive expiration
- Helps keep alveoli patent
- Losses with age/disease
Alveolar surface tension forces
- At air-liquid interface
- Surface tension (ST)
a. draws liquids closer together
b. resists increase in surface area
 | |
| Law of Laplace |
Law of Laplace
- ST directs force/pressure to centre of bubble
- Consequences: small alveoli may have greater P, may create pressure gradients between opposing alveoli causing 'lung instability'
Surfactant
 - Phospholipid produced by type II cuboidal alveolar cells
- Phospholipid produced by type II cuboidal alveolar cells- More concentrated in smallest alveoli
- Sighing replenish levels
- Prevents small alveoli emptying into larger ones
- Prevents collapse of alveoli
- Keeps lungs dryish (osmotic>hydrostatic pressure)
- Reduces surface tension and increases total lung compliance
- Increases lung 'stability'
- Reduces work of breathing
Surfactant: Pathophysiology
- Adequate levels 6weeks before birth
- NRDS - requires +ve pressure breathing and synthetic surfactant
- Levels reduced by alveolar damage and increased macrophage activity
- Energy is needed to overcome 'elastic resistance' of lungs and thorax.
- Posture: lying=decrease in compliance
- Disease: if FRC is increased, Cl is increased and vice versa
So lung compliance is affected by?
- Fibrosis - decrease
- Oedema - decrease
- Age - decrease
- Airway blockage - decrease
- Emphysema - increase
Airway Resistance
- Gas flow proportional to pressure gradient and inversely proportional to resistance
- Poiseuilles Law
Resistance proportional to length (L) and viscocity (η) and inversely proportional to Radius (R)
R proportional to Lxη/r^4
If radius = 1:1/1^4 => R=1
If radius = 2: 1/2^4 => R=
Therefore double the radious = 1/16th the resistance and vice versa
- Radius is primary source
- Trachea and bronchi (rigid and small XS area) = 90%
- Bronchioles=10% (large XS area)
- Narrowing of smaller airways
problems depends on number affected and collapse
Brionchioles
- Reflex control by PSNS and hormones
- Local control by paracrines

Topics to be discussed now in greater detail:
- Gas pressures and gas exchange (recap - above)
- Types of ventilation
- Ventilation and perfusion
- Factors affecting gas exchange
Remember composition of atmospheric air
O2 20.90%, 0.2090 (fraction), 159mmHg (partial pressure)
CO2 0.04%, 0.0004, 0.3mmHg
N2 78.60%, 0.7860, 597mmHg
H20 0.46%, 0.0046, 3.7mmHg
total 100%, 1.0, 760mmHg
in reality there are some other components in the air as well but in very low concentrations that we can actually neglect
Partial Pressure: the partial pressure of any gas can be calculated by multiplying Pb by the fraction of the gas
Example:
PO2=760x0.2090=159mmHg
PN2= 760x0.7860=597mmHg
(missing 5th slide of pulm3 BS2049 module)
Composition of alveolar gas
- Affected by:
Ambient air composition and flow, gas exchange, mixing of gases, humidity

- Upnea
- Hypernea
- Hyperventilation
- Hypoventilation
- Tachypnea
- Dyspnea
- Apnea

V/Q matching
 - Local mechanisms adjust for poor air flow and/or poor blood flow
- Local mechanisms adjust for poor air flow and/or poor blood flow- Capillaries collapsible
- Regulation of arterioles and bronchioles
Va/Qa ratio
- Alveolar blood flow decreases from base to the apex
- Ratio = 3.0 in apex and 0.5 in base
- Average = 0.8
- (Va=5L Qa=6L)
 - Perfusion > Ventilation at rest
- Perfusion > Ventilation at rest

Above we discuss: partial pressures, effects of breathing pattern, defining types of ventilation, effects of hyper/hypoventilation on PAO2/PACO2, V:Q matching, local control of air and blood flow
Topics
- Fick's law of diffusion
- Oxygenation of blood in pulmonary capillaries
- Gas exchange: problems

Types of Hypoxia:
- Hypoxic: low arterial O2
- Anaemic: low HbO2
- Ischemic: low PO2 delivery
- Histotoxic: low O2 use

Fick's law of diffusion:
Diffusion is proportional to:
- partial pressure difference (gradient)
- surface area
Diffusion is inversely proportional to:
- membrane thickness
- diffusion distance
 Gas exchange: Problems
Gas exchange: ProblemsCause hypoxia and hypercapnia:
Inadequate:
- O2 in alveoli
- Transfer of O2 from alveoli to blood
- Transport ....
Gas exchange: Inadequate O2
- abnormal air
- inadequate alveolar Ve
Gas exchanges: inadequacies in tranfer
- decrease in SA for exchange
- increase in thickness of membrane
- increase in diffusion distance




Some essay-question that are seen in exams:
- The impact of emphysema on respiratory function
- Gas exchange: loss of alveolar tissue; decreased SA for gas exchange, loss of traction>obstruction of airways, gas trapping>diffusion gradient affected
- Local regulation of ventilation and perfusion (V/Q) in the lungs
- Mechanics that regulate ventilation and perfusion (V/Q) in the lung
- Factors that affect the efficiency of gas exchange in the lungs
- Factors that affect lung mechanics and gas exchange in health and disease
- Factors that affect the efficiency of gas exchange between the lungs and blood

Respiratory control
now we have done this above but we will extend abit further on some things particularly on exercise (just abit)Neural and chemical control of ventilation
- the main areas of the brain responsible for normal control of normal ventilation
- chemoreception and other influences
- responses during exercise
 | |
| CONTROL CENTRES |

Respiratory control during exercise:
- The Oxygen uptake response
- Ventilatory control:
- mechanisms
- relationships with energy demand
 |
| The oxygen uptake response for a constant workload |
Aerobic metabolism
- Supplies 100% of energy requirements to match low to moderate demands
- Processes are rate limited
- Relatively slow to adapt
- Supported by anaerobic processes to meet demand at the start
- Supported by anaerobic processes to meet demand for moderate to heavy demand.
Ventribular control during exercise
- Associated with combination and/or simultaneous effect of:
a. chemical factors
b. neurological factors
 |
| The Ve response for a constant workload |
We can see three different states at right curve for a constant workload
Non-Chemical control
- Ve rises instantly when exercise starts followed by a short (<20s) plateau
- Ve rises then rises slowly until 'steady state' is reached
- When exercise stops Ve falls abruptly to ~40% of end-exercise value; therefore other control mechanisms are involved
Neurogenic Factors
- Cortical and peripheral
- Neural flow from motor cortex and centres involved in anticipation stimulate respiratory centre
- Sensory input from joints, tendons and muscles adjust Ve during exercise (mechano-reflex)
- Temperature has slow effect
Chemical Control
- Cannot fully explain total rise in Ve
- PaO2 in exercise does not stimulate Ve
- During light-moderate exercise (<2L/min) PaO2 and PaCO2 maintained at normal levels
- In hard exercise CO2/H+ provide stimulus to increase Ve via chemo-R. But PaO2 and PaCO2 maintained at approximately normal levels by ventilation and chemoR on arterial side?
- Ventilatory response slightly lags behind rise in CO2 and H+
- And/or other sensory info exists (from muscle)?
Therefore the Current model of response:
Phase I
Neurogenic stimuli from cerebral cortex and limbs cause abrupt rise/fall in Ve
Phase II
After a short plateau Ve rises to a steady level that meets demand of metabolism intrinsic medullary control and peripheral stimuli modify rate
Phase III
'Fine-tuning' of Ve via peripheral sensory feedback (temperature CO2/H+,K+)
 |
| The Ventilatory Threshold (Tvent) |
Ventilation and energy demand
- Light - moderate exercise:
Ve increases linearly with VO2. Mainly by increases in tidal volume Ve/VO2 ratio indicates breathing economy (ventilation for a given volume of oxygen utilized VO2)
Healthy = 25 (25L air/L VO2)
- Moderate - severe exercise
Ve increases nonlinearly with VO2. Mainly by increases in tidal volume and RR. Ve/VO2 ratio=~35 in severe exercise. 'Ventilatory threshold' (Tvent) also called the 'anaerobic threshold' relates to 'additional' CO2 and H+ from lactate production stimulating chemo-R
Congratulations for you blog! I'd like to know the source of figures (a,b,c,d,e) from "gas exchange". Thanks, Valentina Chakr, paediatric pulmonologist in Brazil.
ReplyDeleteNormal Respiratory Rate can be estimated by measuring how much we use oxygen.
ReplyDeletePretty good post. I just stumbled upon your blog and wanted to say that I have really enjoyed reading your blog posts. Any way I’llbe subscribing to your feed and I hope you post again soon.
ReplyDeleteGood information in this blog Please visit here:
" air ventilation system for home"
" air ventilation system"
" air ventilation"
" air vent system"
This blog is so nice to me. I will keep on here again and again. Visit my link as well..
ReplyDeleteGastroenterologist
If I liked your article, I would have had gastroenterologist related disease before, but now I am tired
ReplyDeletebest gastroenterologist near me
I am hoping same best effort from you in the future as well. In fact your creative writing skills has inspired me.
ReplyDeletehttps://dynamichealthstaff.com/nursing-jobs-in-uk-for-indian-nurses
Bluetooth Smart Watch With Camera And Sim Card Slot Shop Our Official Weekly Ad For The Best Deals Buy phone accessories online At Best and Best Buy has a wide selection of cell phone accessories including cases, chargers, cables,Buy mobile phone bracket online memory cards, adapters and electronics product and much more. You can shop by type of accessory or Onkyo 5.1-Channel HT-S3900 Home Theater System With Bluetooth Buy phone cases online shop accessories by device, including an Shockproof Silicone Case With birleys-electronics And Hand Strap For External DVD Player Plug In To Laptop Via USB 3.0 CD Read/Write Burner Drive accessories, and cell phone accessories for other .
ReplyDeletePuppawradise has been Buy dog accessories online trying out the new self grooming cat brush and bath bag online with our two dogs and three cats and we have found a of many reasons you should consider a waterproof bed sofa house for your pet home.
ReplyDeleteBuy cat accessories online, Buy dog toys online, Buy cat toys online, Buy small pets carrier online, Buy small pet toys online, Buy self grooming cat brush, Buy pet dog beds online, Buy cat bath bag online, Buy arch cat massager, Rechargeable electric pet hair trimmer, Buy Pet nail grinder clippers, Pet grooming glove for dog, Dog grooming glove silicone brush, Plaid adjustable dog collars, Cat carrier travel backpack, Buy Cat bed sofa house, Cat simple grooming glove, Nail clippers toe claw trimmer, Mesh cat grooming bath bag.
buy baby nail trimmer online now. Discount with Free shipping.
ReplyDeletenice http://tsbiomed.blogspot.com/2012/12/notes-in-respiratory-physiology.html
ReplyDeleteAirPhysio is actually a device designed for those who are struggling with respiratory troubles. It is the only gadget that promotes lung capacity and inhaling successfully. The cost for this device is very inexpensive for absolutely everyone. Much better is to click this link https://sites.google.com/view/kuitkel/home or pay a visit to our endorsed site to understand more related to AirPhysio.
ReplyDeleteHey, I saw your post and it is really amazing but I want you to read mine also Airphysio Review
ReplyDeleteThanks for sharing this valuable content with us - Airphysio for children review
ReplyDelete